How is Covid-19 impacting people living in, or at risk of, poverty in Zimbabwe? What policies are needed to mitigate the impact of Covid-19 on chronic poverty? CPAN’s Covid-19 Poverty Monitor is an ongoing research project that interviews people about their experiences of the pandemic. This is the first bulletin focused on Zimbabwe - to find out more about the project, visit our blog about the global project. This bulletin dives into the main economic, health, food security and other concerns of those interviewed, as well as policies to minimise the impacts of Covid-19 suggested by the respondents.
Key Findings
Poverty: Extreme poverty increased from 30% in 2017 to an estimated 49% during the pandemic. (Estimation based on ZIMSTAT’s 2020. Rapid PICES Phone Survey of July 2020, cited in the World Bank (2021). Zimbabwe Economic Update. Overcoming Economic Challenges, Natural Disasters, and the Pandemic: Social and Economic Impacts. June 2021, Issue 3. The World Bank Group.)
Economic vulnerability: The groups at risk of impoverishment due to the Covid-19 pandemic are the chronically ill, women, school children, youth, farmers and semi-skilled workers (formal and informal sector).
Areas of concern for the poorest:
Economic: loss of remittances; price inflation for key goods and services; limited transport; constrained access to markets and widespread job losses.
Health: increased pressure on already stretched health systems, with restricted access to medical treatment during lockdowns.
Food insecurity: increased, with households reducing meals consumed, quantity and quality of food.
Social: upswing in social harms, with increased drug abuse, early sex and teenage pregnancy, commercial sex work and gender-based violence.
Zimbabweans face compound and sequenced shocks, with Covid-19 just one of many negative shocks and trends: People have endured the impacts of prolonged economic and policy shocks, compounded by the effects of climate shocks and harvest failures, price shocks and livestock diseases. This has led to previously resilient households becoming progressively more vulnerable as they move sequentially through preferred to less preferred to highly adverse coping strategies, which ‘mine’ human, social and productive capital, as households prioritise survival.
Adverse coping is widespread: These can have negative consequences for long term health and both social and economic recovery. Examples include engaging in commercial sex work (health impacts, impairs social capital), increased artisanal mining (drudgery intensive, physically dangerous), distress sales of livestock (loss of stores of value, status and ploughing pairs), increased criminal activity (theft, which impairs trust and social capital).
The most widely adopted coping strategy was reported as reducing the number, size and quality of meals. Others included adopting barter trade, reducing cultivated area, distress sales of livestock, livelihood diversification, urban agriculture, sub-letting urban homes, and reverse migration from urban to rural areas.
Mitigation programmes:
Social protection: temporary food aid, social cash transfers. Low coverage during the pandemic – government support (15%) plus NGO support (7% of respondents in the ZIMSTAT Rapid PICES Monitoring Telephone Survey (4th Round) May 2021).
Economic: economic recovery and stimulus package, plus the pre-existing Government conservation farming programme, Pfumvudza/Intwasa, which distributed agricultural inputs to 51% of all households (of respondents in the ZIMSTAT Rapid PICES Monitoring Telephone Survey (4th Round) May 2021).
Groups at risk of impoverishment due to Covid-19 pandemic
The pandemic was one amongst several negative shocks and trends. People who were previously resilient have been forced by a series of idiosyncratic (household-based) and covariant (society-wide) shocks (including economic, policy, climate change, harvest failure and livestock disease-related) to move through preferred to less preferred and then to adverse forms of coping to meet basic needs even minimally. They have become progressively more vulnerable as their asset base is eroded. Some groups have been at particular risk of impoverishment due to the Covid-19 pandemic.
Chronically ill
Older people, people living with disabilities and chronically ill people are highly vulnerable to livelihood and wellbeing declines.
People on antiretroviral (ARV) treatment are worst affected as travel restrictions prevented travel to clinics, so some lost access to medication. However, in some cases, clinics organised local group deliveries, while other patients walked to clinics.
Women
Women relying on remittances: Migrants (usually husbands or partners) reduced or stopped sending remittances.
Female cross-borders traders: Border closures during 2020 and 2021 lockdowns stopped traders from accessing goods, destroying livelihoods.
School children
School and college closures, public examinations missed, few able to access online learning (internet data unaffordable, many did not own laptops or smartphones), private extra lessons too expensive for poor, and private colleges (offering catch up lessons) are also expensive.
Many school dropouts.
Back in school, children are often promoted to the next grade, without having knowledge gaps filled.
Youth
Enterprises owned by, or employing, youth (non-farm, artisans in services sector, semi-skilled workers) were seriously curtailed by lockdown measures.
Farmers
Some farmers have been driven into distress coping, experienced downward mobility and have, so far, completely failed to recover. They were not able to re-stock, unlike those farmers who did not have to sell their livestock.
Reduced market access due to lockdown, resulted in produce spoilage, loss of income.
Reduced agricultural extension support (government and NGOs).
Lack of veterinary services led to increased livestock deaths. Some farmers have failed to recover from livestock losses.
Semi-skilled workers (formal and informal sector)
Job losses due to Covid-19 lockdowns, included factory workers, informal traders, bus conductors, drivers and hairdressers.
Areas of concern for the poorest and potential impoverishment

Loss of remittances, especially from South Africa, drove many households into destitution. This occurred in Tsholotsho District (Matabeleland North Province), for example, where the majority of households relied on remittances before the pandemic, with receipts funding food and education expenditures. Reduced remittance flows reduced household wellbeing and drive school dropouts.
According to the Rapid PICES Monitoring Telephone Survey (Rapid PICES) Round 4, May 2021, about 11% of households nationally received remittances from abroad at around the time of the survey. This is an increase from 9% from the third round, from 5 December 2020 to 10 March 2021 (ZIMSTAT (2021); Rapid PICES Monitoring Telephone Survey (4th Round) May 2021). Although the total percentage of people receiving remittances is not known, as often informal channels are used, a study in 2006 estimated that 50% of the Zimbabwean population received remittances.
Price inflation for key goods and services (including food and agricultural inputs, transport, school fees) have made life tough for many. In Bindura District, (Mashonaland Central Province), for example, between 2019 and 2021, inflation saw prices for groceries and other essential commodities rise by 200-300% and for transport by 100-150% (reported by the local traditional leader).
“We used to pay $1 from Manhenga to Bindura town, but now we are paying $2 to $2.50.”
Transport bans compounded price inflation, with scarcity driving up prices of essentials such as cooking oil and bread by over 60% and maize prices nearly doubling between 2019 and 2021. Illegal transport operators tried to get around the bans, but their fares were too expensive for ordinary Zimbabweans (reported by both female and male farmers in Bindura). Price increases caused tensions, with some respondents believing that retailers were taking advantage of the pandemic to increase their prices.
Farm input costs also doubled, and some farmers were driven to sell livestock to pay for the fertilisers and seed maize they needed to keep farming.
Constrained access to markets (including market closures due to Covid related public health measures) meant that perishable produce spoiled, leading to farmers losing income. With national and international supply chains disrupted, some local markets became flooded (e.g., maize, sweet potatoes and tomatoes) driving prices down significantly.
Widespread job losses (formal and informal sectors) were driven by the lockdown measures. Many chronically poor people, across all the sites, both rural and urban, relied on casual labour for their livelihoods. However, due to the Covid lockdown restrictions, opportunities in the casual labour markets drastically decreased, often resulting in destitution.
Ngwabi (21-year-old from Tsholotsho, who looks after his three younger siblings while his parents were in South Africa) says that casual labour was a source of both food (cereal, cooking oil) and cash for the family. The casual labour activities they undertake include fencing of fields, digging farming holes, slaughtering cattle as well as in community construction projects, such as community infrastructure (e.g., boreholes and dip tanks). However, during 2020 and 2021, there was little demand for casual labour and Ngwabi lamented that:
“Reduced piece job opportunities meant less income for me.”
Some entrepreneurs saw their revenue shrink and some people lost lucrative jobs and had to replace them with lower waged work. For example, Noah (24-years-old, from Nketa, Bulawayo) is an orphan and is responsible for his six dependent siblings. He previously worked at a transport company and earned enough to comfortably cover his household’s expenses. He lost this job and now earns less through his new job, repairing tyres - not enough to cover his family’s needs. He is struggling to maintain household food security and has been forced to add additional strategies, including asking for tips or overcharging his customers, as well as reducing the number of meals to one a day, to ensure their survival.
Cross-border traders were unable to access new stock (groceries from South Africa, rice and second-hand clothes from Mozambique), driving many informal traders and ‘tuck shop’ owners out of business.

Food insecurity increased, with households reducing the number of meals consumed as well as the quantity and quality of food. Diets tended to become less diverse and less nutritious. The Rapid PICES Round 1 survey revealed that 41% of the extreme poor went without eating for a whole day. Urban households who have seen a decline in their incomes have been particularly severely affected.
Bradley (42-years-old, married with three children and two adult dependents) from Bindura reported that he is living hand to mouth. In April 2020 he lost his job at a gold mine and is now doing subsistence farming on two hectares of land. However, he has limited farm equipment and inputs to make the land productive. He has been food insecure since April 2020 and he can hardly find enough money to put food on the table. Others indicated that they sold their small livestock (chickens, goats) to buy food for the household. These distress sales were driven by a collapse in incomes and an increase in costs. Increased food prices and school closures have meant that children are home all day, increasing household food costs, as well as adding to the care burden of the parents.

While Covid‑19 accelerated the use of digital platforms in delivering education, evidence from the Rapid PICES Monitoring Telephone Survey shows that only 25% of rural school-going children continued accessing education after the school closures of 2020, compared to 70% in urban areas.
“Imagine how difficult it is to get income let alone getting enough to buy data bundles to allow the children to do online learning.” Widow, 81, wellbeing category 3, Chitungwiza
Teachers and private colleges provided private tutoring to those children who could afford to pay and who were approaching their public examinations (‘O' levels and A' levels). But the differences between those able to access online learning and tutoring has accentuated pre-existing inequalities.

The pandemic increased pressure on already stretched health systems. Essential services such as vaccinations, maternal and child health services were disrupted as the Government prioritised the Covid-19 response. Around one in four households (19%, rural; 23%, urban) were unable to access medical treatment when needed due to the lack of medical personnel, amongst other reasons (Rapid PICES Round 1 (July 2020)).
Curfews restricted opening times and travel restrictions limited access to health care. This caused a provision gap, with constraints in service provision occurring alongside an increased need for services as some Zimbabwean women and children began to engage in commercial sex work to survive, leading to health risks. However, the government sought to improve staff attendance at government health facilities by providing additional funds (disbursed by the Ministry of Health and Child Care) to motivate and help health front-line workers, including nurses and doctors.
Travel restrictions also led to some people living with HIV and AIDS, especially the elderly who could not walk to the clinics, or pay for illegal transport, losing access to medication:
"Yes, people have been impacted negatively by Covid-19, especially those on antiretroviral drugs (ARVs). They face challenges in accessing their drugs from the Manhenga district council clinic due to lockdown, social distancing and the ban on transport movement. So there have been so many people who defaulted on their daily ARV drugs and this is a health concern during the Covid-19 era." Health worker, Bindura
Relatively few people have been directly affected by Covid-19 in rural Zimbabwe. A small minority contracted Covid-19 and some others faced the grief of having close relatives die of it. For example, Natalie lost her husband and two adult children to Covid-19, with the three dying within six months of each other (see Case study: Natalie).
The vaccination programme was country-wide, reaching even the remotes areas, targeting mainly those over 18 years (Zimbabwe’s population was relatively young, and children (defined as girls and boys under the age of 18 years) constituted 48.8% of the total population (ZIMSTAT, 2013, Zimbabwe National Census, 2012). During a focus group discussion with local authority officials in Bindura Rural District, they estimated that approximately 80% of the adult population in Bindura District had been vaccinated, and they indicated that the Ministry of Health and Child Care have a programme to mop up the remaining 20%. Generally, vaccine hesitancy was low, although there were isolated cases of ‘doubters’:
“I cannot be vaccinated personally even if the government is saying it is compulsory, this vaccination thing is an experiment and trial. They want to experiment on us.” Woman, 34, wellbeing category 4, Bindura
Some people who caught Covid-19, or who contracted serious influenza, reported using home cures and herbal remedies (Indigenous plants were widely used as herbal teas, e.g., moringa and zumbani (Lippia javanica), which is high in zinc and antioxidants), especially those from poor households who could not afford health care. Many feared being tested for Covid-19, because of the damage that a positive test result, and quarantining would do to their earning power. In addition, the hospitals were not prepared to handle the rapid increase of Covid-19 cases and resources were stretched very thin.

There has been an upswing in social harms during the pandemic, with increases in gender-based violence (GBV), drug abuse, early sex and teenage pregnancy and commercial sex work. Anecdotal reports indicate that crime rates have increased during the pandemic, particularly theft. Lockdown measures have been associated with severe psychological distress.
Gender-based violence (GBV) has increased, associated with families being in a confined space for long periods during lockdown (household food insecurity, increased unemployment and financial worries, compounded by male anger, anxiety and frustration and women’s diminished agency and means of escape). The rise in incidence appears to be particularly high in urban areas, where homesteads are small.
School closures, lasting nearly two years, have had far-reaching negative impacts. Some children from richer families were able to access online learning or work with private tutors but children from poorer families were unable to access learning. Some children worked for their parents, helping them farm or in the family business. However, widespread ‘idleness’ amongst young people has been associated with an increase in early sex, leading to an increase in STIs and teenage pregnancies.
Drug use, especially amongst the youth, increased during the lockdown. The main drugs used by poor youth are marijuana (about 80% of drug users) and crystal meth (methamphetamine), with more affluent youth using cocaine and heroin. Some cough medicines are used as drugs, particularly by the extremely poor youth (e.g., BronCleer, manufactured in South Africa, and containing codeine and alcohol). The government has created a Drug and Substance Abuse Technical Working Group led by the Ministry of Public Service, Labour and Social Welfare. This is an information-sharing platform between Government and relevant stakeholders and has been tasked with reducing the effects of substance abuse. It was established under the Government’s National Drug Master Plan for tackling youth substance abuse.
Crime rates have increased, particularly theft, with burglary increasing significantly in our four study sites (Bindura, Bulawayo, Chitungwiza and Tsholotsho), driven by increased youth unemployment, return migration from South Africa and poverty. This has occurred alongside an increase in customers for stolen goods.
Psycho-social impact of Covid-19 restrictions: Restrictions around social gatherings including funerals have meant that grieving families have been unable to seek comfort through social contact and traditional funeral rites. The inability of families to bury their dead, and particularly transporting the bodies of those who have died in urban areas to the person’s ‘rural home’ for burial, has caused great distress.
Government containment measures
Covid-19 lockdowns: The first Covid-19 lockdown in Zimbabwe was announced on 17 March 2020, when a national disaster was declared. The lockdown eased towards the end of the year, as new cases and deaths decreased. However, there was a spike in January 2021, probably due to opening the borders with South Africa, as well as an increase in social gatherings around the festive season. There was a second major lockdown from 5 January 2021 to 1 March 2021. By September 2021, infections had declined significantly and restrictions were relaxed to Level 2 in October 2021. The lockdown levels are Level 4, very high; Level 3, high; Level 2, moderate; and Level 1, low. Throughout the Covid period, Zimbabwe had two main Levels of lockdown restrictions, namely Level 4, the most severe and Level 2, which was more relaxed. Lockdown restrictions were eased, with the ban on intercity travel removed, business hours extended from 8 pm-7 am and a shorter curfew, from 10 pm-5 am. Public gatherings of up to 100 people and international travel were allowed.
Then, with the emergence of the Omicron variant of Covid-19 in December 2021, the Government imposed another strict (Level 4) lockdown to cope with the rapid increase in infections. This meant that businesses could only operate between 8 am-3.30 pm, the curfew was extended from 6.30 pm-6.30 am and limits were imposed on public gatherings, with a maximum of 30 people at a funeral. This was initially imposed for two weeks, then extended. However, by February 2022, cases had greatly declined and the lockdown was eased back to Level 2.
The lockdowns included:
A nationwide curfew;
A stay-at-home order with exemptions for those working in essential services;
All formal enterprises and registered informal enterprises ordered to cease operations;
Inter-city travel banned;
Closure of borders and non-essential businesses;
Gatherings except for funerals were banned;
Schools closed, except for some examination classes.
In addition, there were preventative public health measures, which included requirements that the public wore facemasks correctly and complied with social distancing, hand sanitisation and temperature checks (Government of Zimbabwe (2021)). These preventative health measures were required for all lockdown levels.
Quarantine centres for international returnees were established by the Ministry of Public Service, Labour and Social Welfare in some Provinces, particularly those with borders, such as Matabeleland South. Several were established in Harare and Bulawayo and used schools and colleges facilities.
School closures: By mid-March 2020, there were many reported cases of Covid-19 in schools, and some individual schools closed. On 24 March 2020, Government announced a nationwide closure of schools and tertiary institutions, to contain the spread of Covid-19. Schools remained closed until September 2021 and by December 2021, another strict lockdown was in place. Schools remained closed in January 2022, with exemptions for examination classes. By February 2022, the Omicron threat had subsided, and schools reopened on 8 February 2022. Approximately, 4.6 million children have been affected by the Covid-19 closure of schools in Zimbabwe. (21 February 2021. Chipenda, C., and Tom, T., (2021) Zimbabwe’s Social Policy Response to Covid-19: Temporary Food Relief and Cash Transfers; Global Dynamics of Social Policy. CRC 1342 Covid-19 Social Policy Response Series No. 23. Bremen: University of Bremen).
Vaccination: The national Covid-19 vaccination programme launched in February 2021 (organised by the Ministry of Health and Child Care), using the Sinopharm BIBP vaccine (Sinovac and Sputnik V were also used). Vaccinations were made compulsory for State employees to reduce the risk of spreading Covid-19 to others. Those who were unwilling to be vaccinated, due to religious reasons or vaccine hesitancy, had to resign.
Livelihood groups particularly affected by travel restrictions: Farmers and traders. Venders indicated that they had experienced police harassment.
Penalties: People could be fined by local traditional leaders and arrested and fined heavily by the Zimbabwe Republic Police. At the district and national level, the fines for offenders were reportedly ZWL 500 ($1.38) (all currency conversion as of 26 February 2022 using xe.com) to ZWL 10,000 ($27.63), depending on the offence. Those caught without wearing masks in a rural village could be fined a goat or a bucket of maize. (KII, traditional leader, Bindura).
Compliance: Compliance with the containment measures was high, with people generally appreciating that this was the only way that the pandemic could be managed, and lives saved. This was supported by clear and educational health promotional campaigns, delivered through television, radio and poster campaigns.
Impact: The government’s strict travel restrictions and curfews had widely reported impacts. Travel restrictions made buying groceries, visiting relatives, or seeking medical treatment difficult, with negative consequences for older people, the sick, vendors, farmers and anyone who needed to access medication, and although district health workers facilitated access to ARVs and other essential medicines, access was patchy.
“The area has experienced strict lockdown measures [affecting] churches, schools, swimming pools and bottle stores. We all try to follow rules. Security guards always made sure that masks were worn properly covering both nose and mouth. Those not adhering to the rules were taken to the police station and made to pay a fine. During the first lockdown days, people used to be taken to the police camp and kept at the police station the whole afternoon and only released at the end of the day and still pay a fine.” Local businesswoman, Nketa, Bulawayo
“During the first lockdown people were not allowed in town at all for the first 21 days. If police officers saw you 5km or more away from your house you were made to pay a fine.” Pastor’s wife, Nketa, Bulawayo
Coping strategies
Diverse coping strategies were adopted, with a reduction in meals cited most frequently (the remaining coping strategies are not in rank order). But as households progressed from preferred forms of coping to adverse coping, social harms increased and the long-term damage to their ability to move back out of poverty intensified.
Reduced meals and less nutritious food: Reducing the number of meals per day was identified by almost all respondents as a key coping strategy (across four districts – rural and urban – and across all well-being categories) in response to the economic crisis induced by lockdown measures. This saw the number of meals reduced from three to two or even one meal a day. Crisis induced food insecurity was so acute for some that everyone in the household would go the whole day without eating and some urban households sought to reduce the number of mouths to feed by sending their children to their ‘rural home’, where they were looked after by grandparents or extended family members.
“I [reduced] the number of meals per day from the three, to two or even one per day when things are very difficult.” Woman, 28, wellbeing category 2, Chitungwiza
“Loss of revenue and reduced meals per day is a major challenge, my family used to have several meals per day without any limits and now I feel like it’s not fair to my wife and kids, I feel like am no longer a man enough for my family.” Male, 50, wellbeing category 3, Bindura
Some households had a less severe response by shifting to consuming ‘inferior foods’ - eating cheaper, less preferred, less nutritious foodstuffs, such as ‘muputi’ (roasted maize kernels).
Barter trade: Barter trade has increased in urban and rural Zimbabwe, and in some areas, such as Bindura (Mashonaland Central Province) and Tsholotsho (Matabeleland North Province), it was reported that cash was rarely seen. Services by artisans, such as builders, as well as casual labourers, were often paid in kind. Payment in kind is quite acceptable and the goods appreciated, especially in the hyperinflationary environment, and where banks restrict cash withdrawals, and in addition, mobile money has various taxes and conditions imposed.
“Some mining families ventured into barter trade. The grocery shop owners would come to the villages with essential commodities and exchange foodstuffs like cooking oil and mealie meal with some grams of gold. This helped most families in coping with the shock.” Traditional leader, Bindura
Reduced area of cultivation: Some farmers reduced the proportion of their land that they farmed, as they could not afford to buy inputs or to pay for ploughing, leading to lower production levels. More farmers needed to buy in ploughing services in 2021 as their draught power was limited by livestock deaths from disease (widespread theileriosis or January disease and blackleg). However, ploughing services were limited and not readily available at the times required for ploughing (AGRITEX (agricultural extension) broadcasts to farmers in each locality, the optimum times for ploughing, depending on the rainfall pattern for that specific year. Usually, this period for ploughing is quite narrow.)
Livestock sales: Distress sales of small livestock (chickens, goats, pigs) became widespread in order to meet contingencies such as buying food and agricultural inputs and paying for children’s school fees and other education expenses.
Livelihood diversification: Livelihood diversification was adopted as a coping strategy by approximately half of the farmers in our study who, for instance, moved into value addition (vegetable drying, tomato preservation). Some rural people harvested thatch grass for sale. Others collected seeds and developed seed banks for themselves and for sale. Some sought casual work. Those with pre-existing horticultural enterprises increased their output, particularly those near a ready market, for example, artisanal mines. Some began brewing beer or selling cigarettes, and others moved into selling marijuana. The number of women, youth and children engaging in commercial sex work also increased, as households sought to cope with job losses and the loss of remittances as a result of the pandemic.
Expenditure prioritisation: Some poor urban households made tough choices around which expenditures to prioritise and stopped paying their rent and utility bills. This meant that they fell into arrears, leading to tension with landlords and the accumulation of debt.
Urban agriculture: Many urban households (for example in Bulawayo) sought to become self-sufficient and began to cultivate vacant plots, green belts and wetland areas in order to produce their own food and rear chickens.
Subletting of urban homes: Subletting was a common livelihood strategy before the pandemic for some non-poor households in Bulawayo and Chitungwiza. However, the proportion of non-poor households subletting increased during the Covid-19 pandemic, as other income streams failed. This included letting rooms in their houses and building backyard shacks to rent out.
Reverse migration: Reverse migration has become common, with urban households sending children or other family members to their ‘rural home’. Sometimes the whole household relocates, to benefit from the lower cost of living and greater opportunities for self-sufficiency through food cultivation.
Community initiatives: Rural chiefs assisted poor and food-insecure families through the Zunde raMambo royal court food initiative. This was to supplement government relief, which was not always adequate. For example, a local Chief in Bindura mentioned that in 2020, the Covid-19 food relief funds from the government were insufficient for all the hungry families in his domain, so his royal court provided extra grain, through the Zunde raMambo initiative.
Programmes in place to mitigate impoverishment due to Covid-19
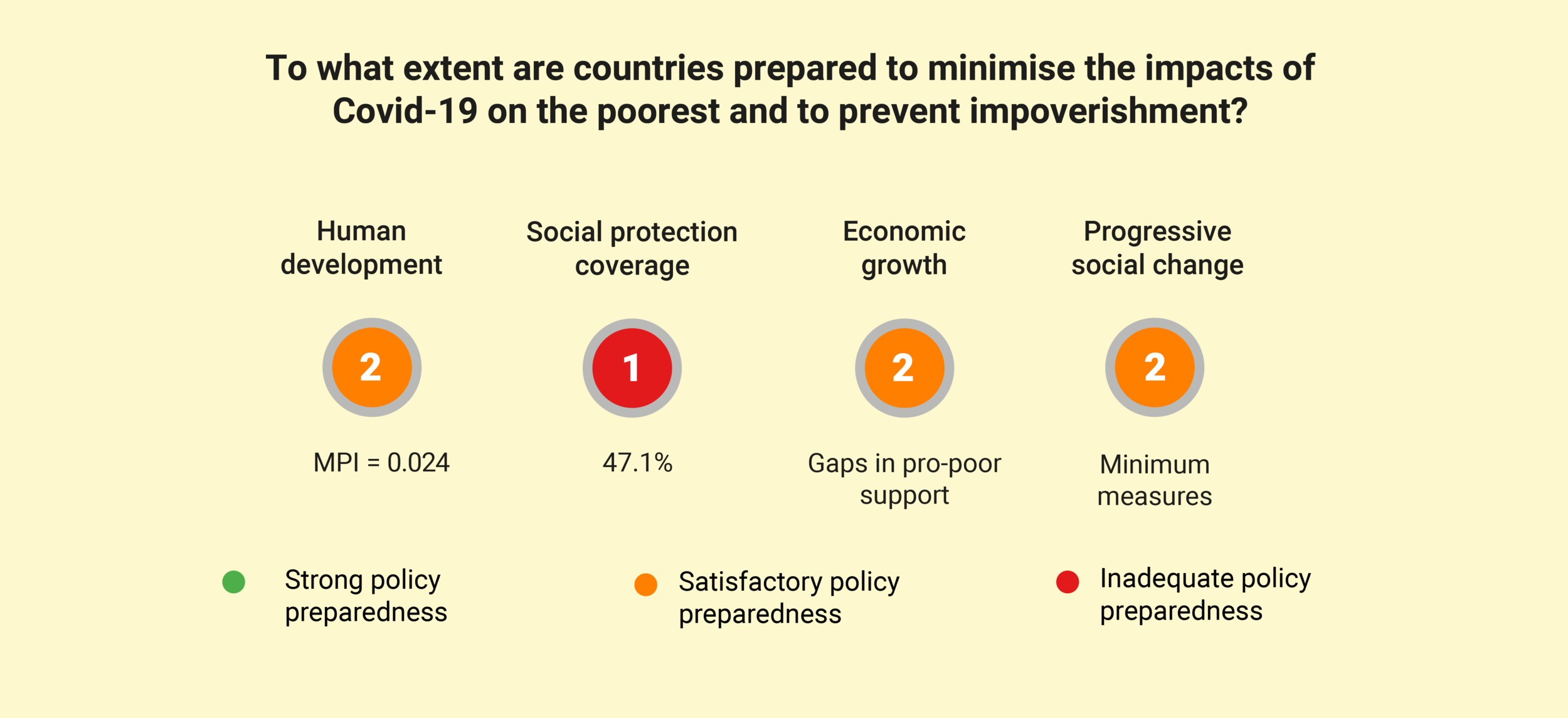
Almost no assistance from the Government or international organisations was reported. The exception was the Government’s Pfumvudza/Intwasa conservation farming programme, which distributed agricultural inputs to 1.8 million smallholder farmers (the Input Package for a Pfumvudza/Intwasa Plot was distributed through the Presidential Inputs Programme and consisted of 2kgs seed, 12kg lime, 16kg Compound D, 16kg Ammonium Nitrate, and insecticide for pests). Fifty-one percent of all households (predominantly rural and peri-urban, although the programme can also be carried out in urban areas where space allows) have participated in the Pfumvudza programme (Findings from the 4th Round of the Rapid PICES Monitoring Telephone Survey). Of these, 84% had received extension services and training and 80% reported higher yields (ZIMSTAT (2021). Rapid PICES Monitoring Telephone Survey (4th Round) May 2021).
Social protection coverage in Zimbabwe was poor before the pandemic. It remained relatively low, with only 15% of respondents receiving government support and 7% support from a non-governmental organisation (ZIMSTAT (2021). Rapid PICES Monitoring Telephone Survey (4th Round) May 2021). This is despite severe poverty levels increasing to an estimated 49% and food insecurity increasing to around 70% (World Bank (2021). Zimbabwe Economic Update. Overcoming Economic Challenges, Natural Disasters, and the Pandemic: Social and Economic Impacts. June 2021, Issue 3. The World Bank Group). None of the participants in Poverty Monitoring Initiative mentioned receiving any social protection support, although a few of those in the destitute wellbeing category mentioned that they used to get assistance from the Department of Social Welfare, but had not received anything for the past couple of years. Several participants, in the very poor category, mentioned that some of their orphaned grandchildren received assistance under Basic Education Assistance Module (BEAM).
Pre-existing support to poor people
Support to agriculture: The Government’s Pfumvudza conservation farming inputs programme, 2020 to 2021, was cited by the majority of respondents for this study as their sole form of external support.
Free health care: at government clinics and hospitals.
Free education: Basic Education Assistance Module (BEAM) provides a school fee waiver to children identified as poor or vulnerable.
Food security: World Food Programme drought relief programme to vulnerable households.
Civil society support: Most churches assist, especially the elderly and destitute. This ad hoc assistance commonly distributes food hampers. In Bindura, the Muslim community mosque stepped in and provided poor households with food hampers.
Covid-19 response
Temporary food relief: Ongoing food aid distribution was scaled up during the pandemic. Distribution of food aid was constrained and the proportion of households receiving food dropped from 23% in July 2020 to 3% in August-September 2020. In urban areas, only 1% received food aid, or cash transfers to buy food, during this period, thus leaving many families food insecure (World Bank (2021). Zimbabwe Economic Update. Overcoming Economic Challenges, Natural Disasters, and the Pandemic: Social and Economic Impacts. June 2021, Issue 3. The World Bank Group).
Social cash transfers: Cash transfers were central in Zimbabwe’s Covid-19 social protection response and by 13 October 2020, the government had provided cash transfers to 202,077 beneficiaries (Zimbabwe’s cash transfer programme was allocated ZWD 2.4 billion ($6.6 million) by the national stimulus package), throughout the country. However, there was a strong urban bias, with Harare (45%) and Bulawayo (15%) having the highest proportion of beneficiaries. Targeting sought to identify the most vulnerable and was based on the Ministry of Public Service, Labour and Social Welfare’s databases supplemented by means-testing with lists from the Ministry of Women Affairs, local authorities and informal traders used to identify new beneficiaries.
Challenges centre around coverage and transfer size. Transfers rose from ZWD 180 ($0.49) to ZWD 300 ($0.82), but this was widely considered inadequate, remaining substantially below the Consumer Council’s reported monthly family basket of ZWD 14,438 ($39.89). In terms of coverage, the proportion of households receiving Covid-19 cash transfers declined from 4% in Round 3 of the Rapid PICES to 1% in Round 4 (ZIMSTAT (2021). Rapid PICES Monitoring Telephone Survey (4th Round) May 2021). This decline was true of both urban and rural areas. Though the reason for the decline remains unclear.
Economic stimulus: In May 2020, the government unveiled a ZWD 18.2 billion ($50.3 million) Covid-19 Economic Recovery and Stimulus Package, valued at 9% of GDP. The aim of the package was twofold. Firstly, it sought to improve the country’s economic performance and ensure recovery from Covid-19-induced shocks. Secondly, it sought to provide relief to individuals, families and businesses affected by Covid-19. It aimed to reach one million households with relief, including food-deficit mitigation, cash transfers, facilitating and financing healthcare interventions, packages to trigger social welfare, pension support, provision of cushioning allowances, and funding state institutions for Covid-19 research and manufacturing of personal protective equipment. The Government provided ZWD 739 million ($2 million) of the Economic Recovery and Stimulus Package to the Ministry of Health and Child Care to fund various interventions, such as a hiring additional 4,000 health personnel; upgrading of and appropriately equipping all central, provincial and district hospitals and other facilities to accommodate Covid-19 patients; and provision of a tax-free allowance for frontline health workers.
None of the respondents in the Poverty Monitoring Initiative indicated that they had heard of, or received, any benefits under the Covid-19 Economic Recovery and Stimulus Package.
Education programmes: Access to online learning was provided during the 2021 lockdown through the UNICEF, Ministry of Primary and Secondary Education and Microsoft’s ‘Learning Passport in Programme’. This digital platform gave teachers and pupils free online access to learning materials, although children’s access was limited by the costs of buying data bundles for internet connectivity and only 4% used mobile learning applications, 2% of children were found to have listened to educational radio programs, 1% watched educational television programmes (Rapid PICES Monitoring Telephone Survey Round 4).
Case studies
Case Study: Natalie
Natalie, a 58-year-old widow living in Nketa high-density suburb in Bulawayo, has been devastated by the pandemic. She lost her husband and two adult children (36-year-old daughter and 29-year-old son) to Covid-19, dying within six months of each other. They were the household’s breadwinners, so her income has collapsed at the same time as her outgoings increased, as she is now responsible for looking after her three orphaned grandchildren.
When her husband and children fell ill, she asked relatives for money to enable them to access medical treatment. Although one child had Medical Aid insurance, it did not cover all the costs and Natalie was also forced to sell assets, including the family car.
Losing her loved ones has been the greatest challenge that Natalie has ever experienced, and she is now lonely, poor and faces the burden of taking care of her grandchildren.
Case study: Thomas
Thomas (now 21 and single) and his three younger siblings (Rachel, 16, Maria, 14, and Joseph, 12) live in a dilapidated homestead in rural Tsholotsho. It is in serious need of repair, with cracked walls and loose thatch on the roof. They are poor and own only one acre of land, five goats, a radio and a small solar panel.
Five years ago, Thomas became his siblings’ guardian when his parents moved to Johannesburg to work as domestic workers. For some time, they sent regular remittances in the form of both money and groceries. Sadly, the remittances have dwindled to almost nothing. Life has been tough for the parents since the start of the pandemic, so much so that they wanted to return to Zimbabwe, but they are stuck as they could not afford to relocate their accumulated assets, including furniture.
Thomas reported that his siblings had had to drop out of school, as they could not afford school fees. They had started helping him with household chores and with cultivating their land. They were not able to return to school when they reopened, largely because the family could not pay the arrears in school fees.
Previously, Thomas and Rachel found casual work around the community, fencing fields, digging holes for planting, slaughtering cattle and on community construction projects, (e.g., digging boreholes and dip tanks). This work provided them with enough income to survive, buying food, enabling them to pay to grind their maize, buy soap and pay for sanitary wear. Unfortunately, casual work opportunities have reduced drastically during the pandemic, leaving the household with very little money. The price of basic goods and services have increased at the same time.
Their farming is rain-fed and prone to waterlogging but they manage to cultivate some pearl millet and sorghum. Although they do not have cattle (and so no draught power), they do have five milking goats. They use soured goat’s milk to make a ricotta-like soft cheese, which they eat with sadza (maize porridge). They also collect thatching grass to sell. Thomas also owns a large number of pigeons, which he uses as a source of protein for the family as well as selling ‘start-up’ birds to neighbours. Rachel earns some income from commercial sex work. She visits a local bar and sometimes comes back late at night with gifts.
The family have had minimal NGO/Government support, and Thomas believes that support is often concentrated on older people, although he comments that some youths are equally vulnerable.
Methodology
This Zimbabwe Covid-19 Poverty Monitor Bulletin is informed by qualitative data collected by the Poverty Monitoring Initiative and the University of Zimbabwe. The interviews for this bulletin took place in November 2021, in four districts (two rural and two urban): namely Bindura Rural District in Mashonaland Central Province; Tsholotsho District in Matabeleland North Province; Nketa suburb of Bulawayo; and Chitungwiza, Harare Metropolitan Province. Ten in-depth semi-structured interviews were conducted in each study site (40 in total) in addition to approximately 20 local key informant interviews.
These data are drawn from the first round of a panel study, with the second round being collected in March 2022. More details on the sampling and methodology for this bulletin can be found here.
This bulletin was created in collaboration with the University of Zimbabwe and made possible with support from Covid Collective.
Supported by the UK Foreign Commonwealth and Development Office (FCDO), the Covid Collective is based at the Institute of Development Studies (IDS). The Collective brings together the expertise of, UK and Southern-based research partner organisations and offers a rapid social science research response to inform decision-making on some of the most pressing Covid-19 related development challenges.

